Overview
We built a tool that estimates how many days a patient will stay in the hospital so the hospital can plan beds and staff ahead of time.
- Hospital management gained urgency during COVID-19, when poor allocation of beds and ventilators caused serious complications.
- HealthPlus hired us to find what drives length of stay (LOS) and predict it from data available at admission plus a few tests.
- Accurate LOS at admission lets the hospital pre-allocate beds, staff, and equipment instead of reacting to overcrowding.
- Goal extends beyond analysis: deliver a model that can actually be serialized and deployed into hospital operations.
Methodology
flowchart LR A[Raw Data] --> B[Clean & Encode] B --> C[EDA] C --> D[Train/Test Split] D --> E["Random Forest / Linear Regression / Ridge / Lasso"] E --> F["Tune (Cross-Validation)"] F --> G["Evaluate: R2 / RMSE"]
The Data
We used records of half a million hospital admissions, each describing the patient, their ward, department, and their actual stay.
- Dataset of 500,000 patient admission records across 15 columns, with no missing values and all rows unique.
- Numeric fields include Available Extra Rooms, staff available, Visitors with Patient, Admission Deposit, and target Stay (in days).
- Categorical fields capture age band, department, ward type, severity of illness, and treating doctor.
- Same patient could be readmitted up to 21 times; ~3 spare rooms and ~5 staff available on average per admission.
- Target is continuous days of stay, so this is framed as a regression problem.
Exploratory Analysis
We looked at patterns in the data and found that the department and ward, not the numeric measurements, explain how long patients stay.
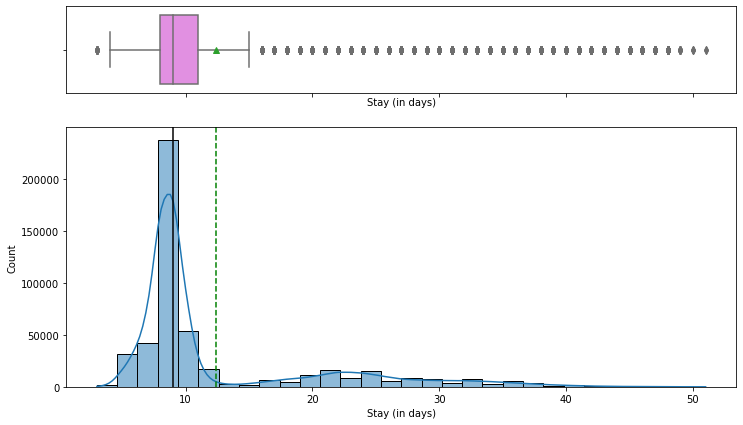
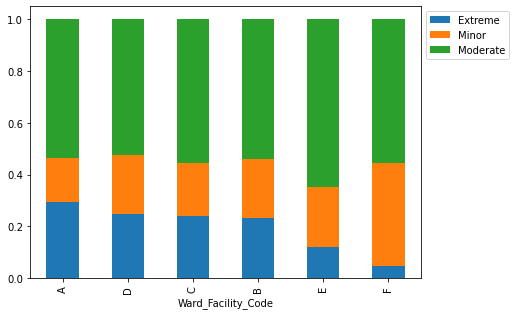
- Most patients stay 8-9 days; few exceed 10 days and very few exceed 40, consistent with mostly moderate or minor illness (~82%).
- Correlation heatmap shows almost no linear relationship between numeric features and LOS, pointing to categorical drivers.
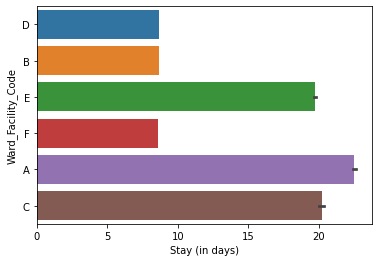
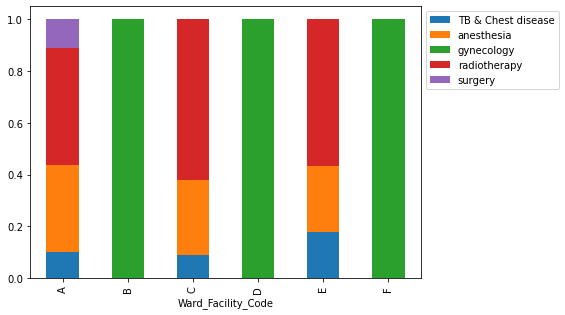
- Wards A and C have the longest stays and house serious cases; Ward A holds the most extreme cases and all surgical patients.
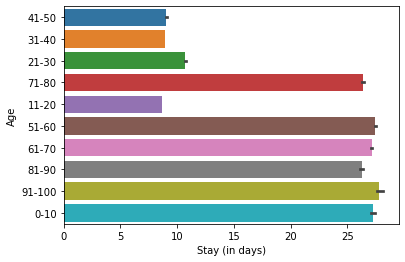
- Gynecology is the busiest department (~68% of patients); patients aged 1-10 and 51-100 tend to stay the longest.
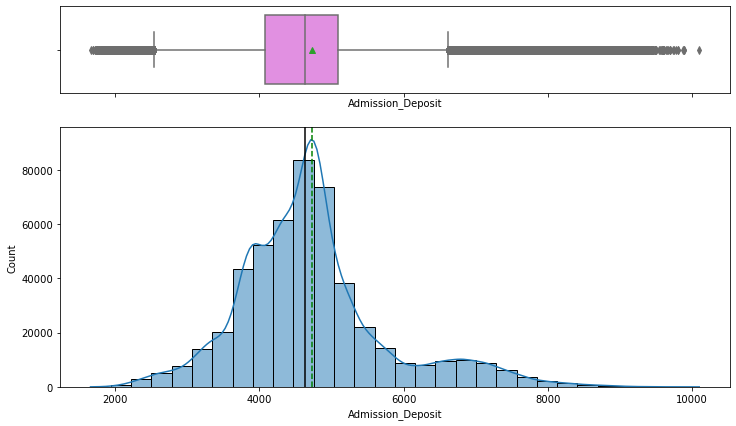
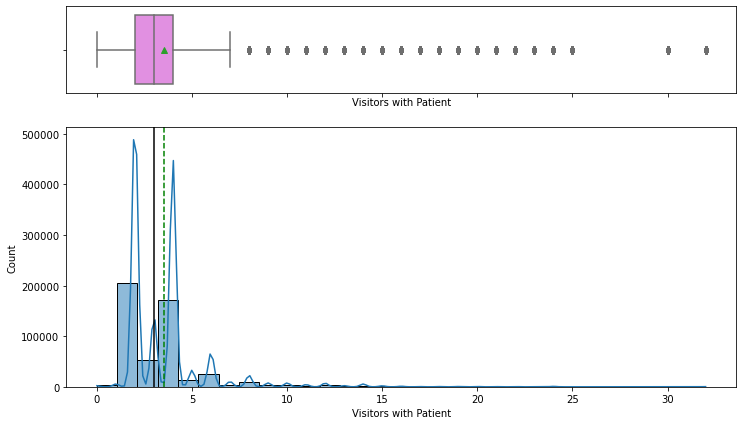
- Admission Deposit is near-normal with two-sided outliers; visitor counts are right-skewed (2 and 4 most common).

Modeling & Results
We tested several prediction methods and a Random Forest, after fine-tuning, gave the most accurate length-of-stay estimates.
- Encoded categorical features, split into train/test, and evaluated with RMSE, MAE, R-squared, Adjusted R-squared, and MAPE.
- Compared Decision Tree, Bagging, Random Forest, AdaBoost, Gradient Boosting, and XGBoost regressors.
- Random Forest Regressor won with the lowest RMSE and MAE; hyperparameter tuning slightly improved its RMSE and R-squared.
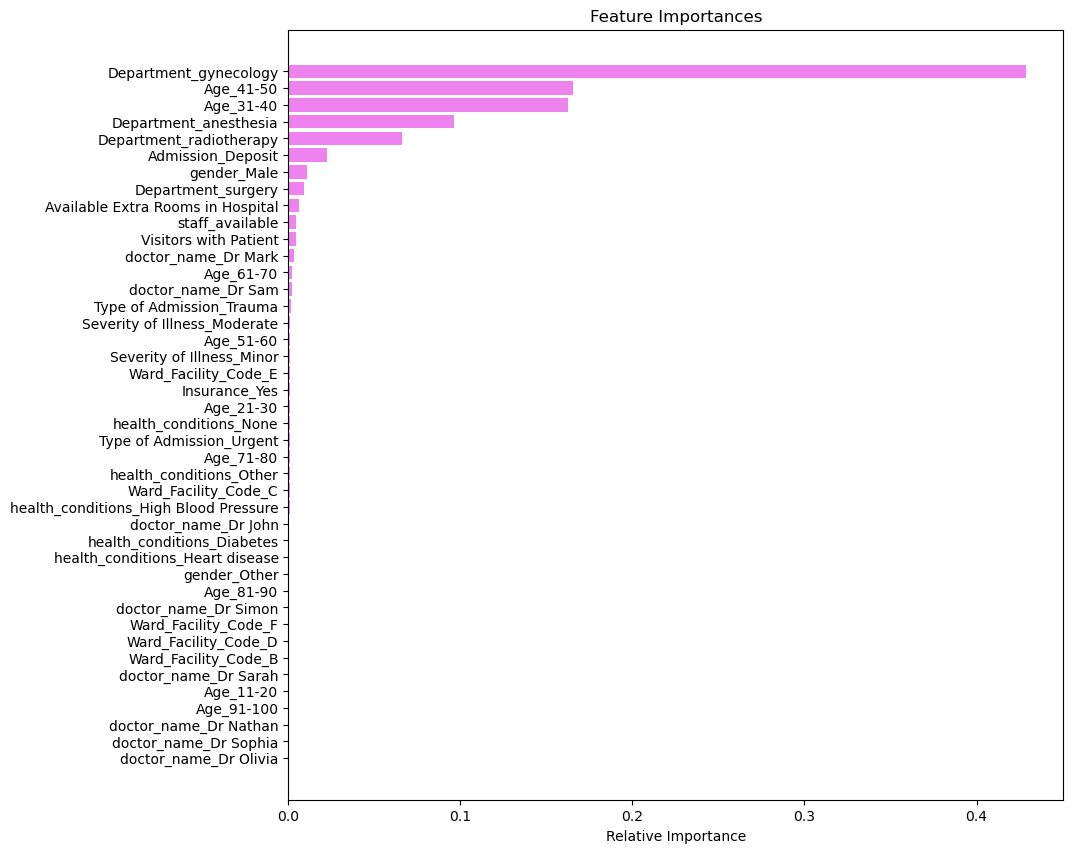
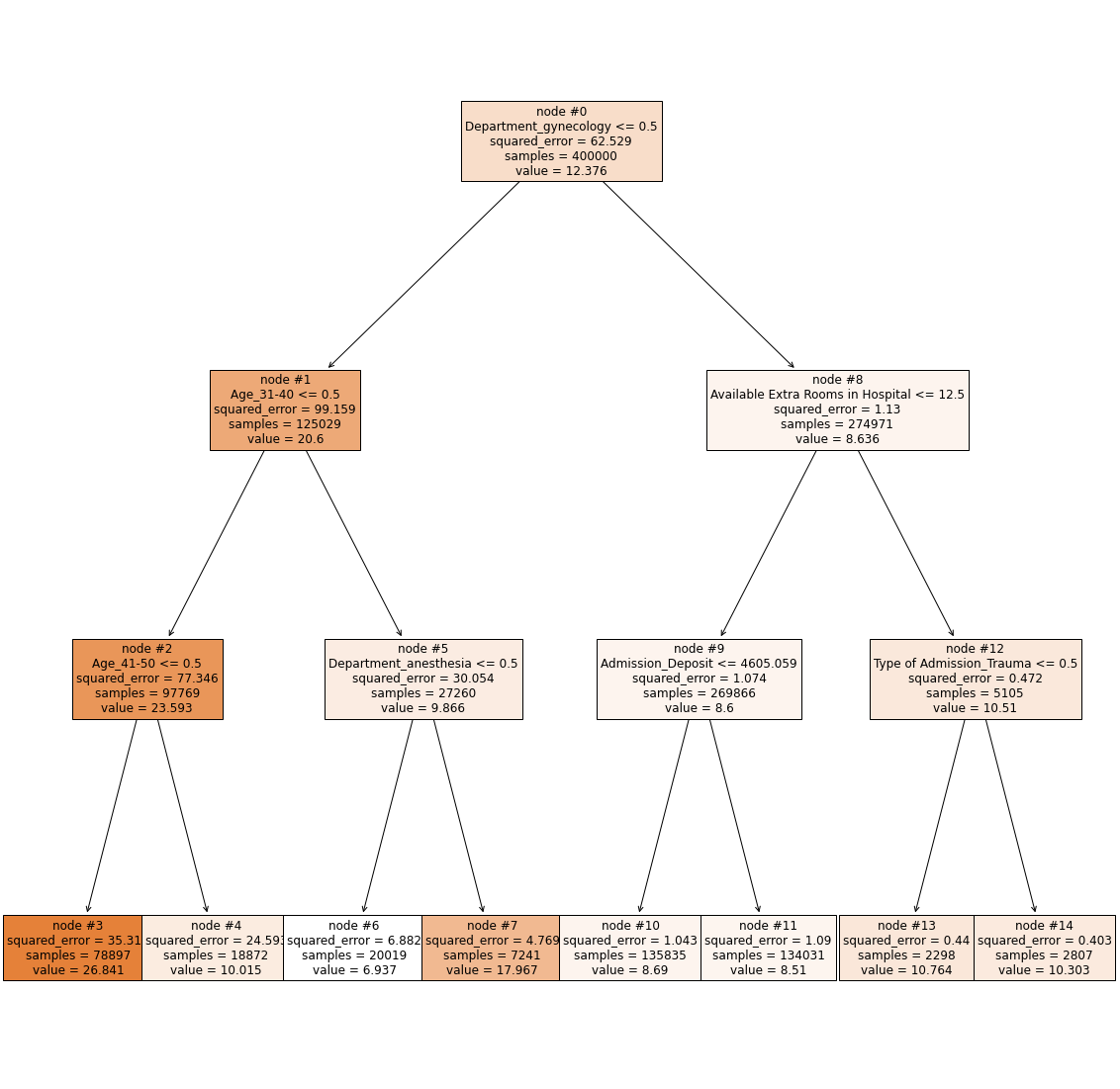
- Decision tree root split on Department=gynecology, confirming department is the highest information-gain feature.
- Top features: Department gynecology, Age 41-50, Age 31-40, then anesthesia, radiotherapy, and Admission Deposit.
Productionizing the Model
We packaged the trained model into a file so it can be saved, shared, and loaded by a live system to make predictions on new patients.
- Wrapped preprocessing and the model in a single scikit-learn Pipeline with a ColumnTransformer so raw admission data feeds straight in.
- Serialized the trained model to disk with Pickle (model.pkl) using pickle.dump, reloaded via pickle.load for inference.
- Also persisted with Joblib (model.joblib), which is more efficient for the large NumPy arrays inside the Random Forest.
- A serialized pipeline can be loaded behind a service at admission to return a live LOS estimate without retraining.
- Pipeline packaging makes the artifact reusable as a starting point for future deployment and further model development.
Key Takeaways
Knowing a patient's likely length of stay at admission helps the hospital staff its busiest departments and manage resources.
- Gynecology handles 68.7% of all patients and needs ample dedicated staffing and resources to run smoothly.
- Department, age band, and ward drive LOS far more than numeric measures, so capacity planning should center on them.
- Tuned Random Forest, served via a Pickle/Joblib pipeline, gives operations an at-admission LOS forecast.
- Visitor counts reach up to 32 per patient; capping visitors is a low-cost operational recommendation.
- Built with: pandas, numpy, matplotlib, seaborn, scikit-learn, xgboost, pickle, joblib
More Visualizations
Tech Stack
- pandas — data wrangling and tabular manipulation
- numpy — fast numerical arrays
- scikit-learn — modeling, pipelines, and evaluation
- seaborn — statistical visualization
- matplotlib — plotting
- xgboost — gradient-boosted trees
Attribution
This project was completed as part of the MIT Applied Data Science Program (MIT IDSS / Great Learning). The program provided the case-study scaffolding; the analysis, code, and results are my own. Published with permission, for portfolio use only.